Designing the Message as Care
How a Jefferson team treated patient communication as service delivery through a reusable Epic message system, visual assets, and a workflow staff could carry across care gaps.
Operating context
Jefferson Population Health
March 2023–January 2024
- Role relationship
- Message-system designer and builder
- Contribution
- I designed and built the patient-message layer: reusable visual assets and Epic message templates, implementation documentation, and staff training. Marketing reviewed brand use, Population Health leadership reviewed operations, and the relevant clinical or program owners retained authority for clinical wording, care-gap requirements, and approval. Copy development was collaborative. The program manager and director managed existing workqueues and data pulls; I did not own eligibility logic, source extracts, workqueue infrastructure, Jefferson's enterprise Epic environment, or clinical policy.
- Result
- A reusable library of roughly 25 message and graphic assets, a tested cross-device receiving pattern, and a repeatable delivery workflow that staff were proud to use. The implementation record does not establish a numeric or causal response effect, patient comprehension, accessibility conformance, or clinical outcomes.
The message is part of the care experience
Patient communication is part of the care experience because it shapes whether a person can recognize, understand, and act on what the organization is asking them to do.
A patient message can be technically delivered and still feel like an afterthought. Important outreach often arrived as a block of administrative text: accurate enough to send, but hard to recognize, scan, or act on while a person was already balancing work, family, uncertainty, or a full portal inbox.
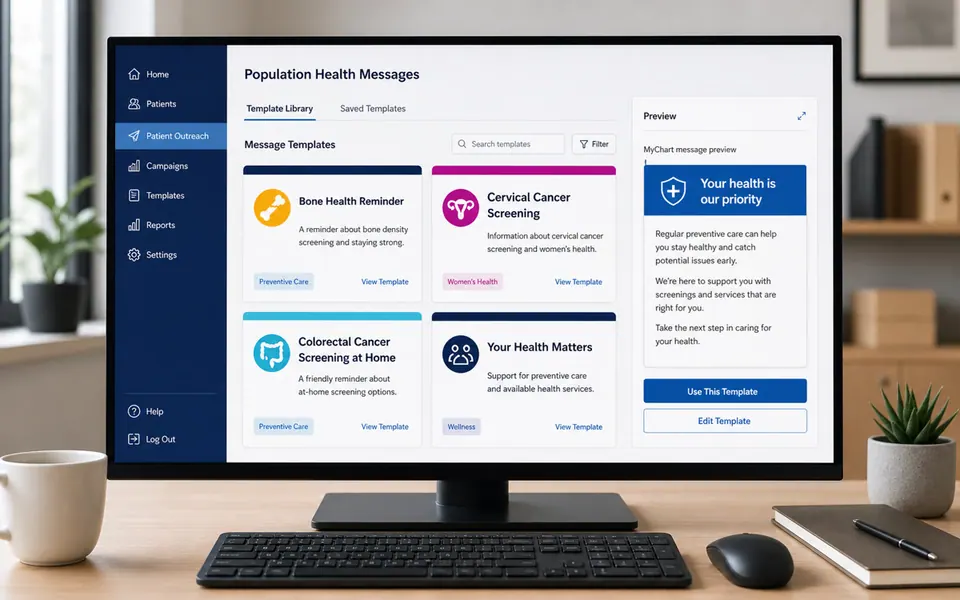
Receiving-experience reconstruction
The same outreach job can arrive with a different sense of care.
A later editorial reconstruction of the cross-device comparison used during implementation. It is not a live MyChart screen, a preserved patient message, or evidence that either treatment changed patient behavior.
During cross-device demonstrations, we compared an ordinary, text-heavy portal message with an action-oriented message that used a recognizable Jefferson visual hierarchy, a clear next step, and companion copy. The comparison made implementation behavior inspectable on phones and computers. It did not measure comprehension, accessibility conformance, trust, response, or clinical outcomes.
That receiving experience was the point of the work, and the image supported the words and delivery path as one deliberate part of a service the patient had to receive and use.
Why the communication layer mattered
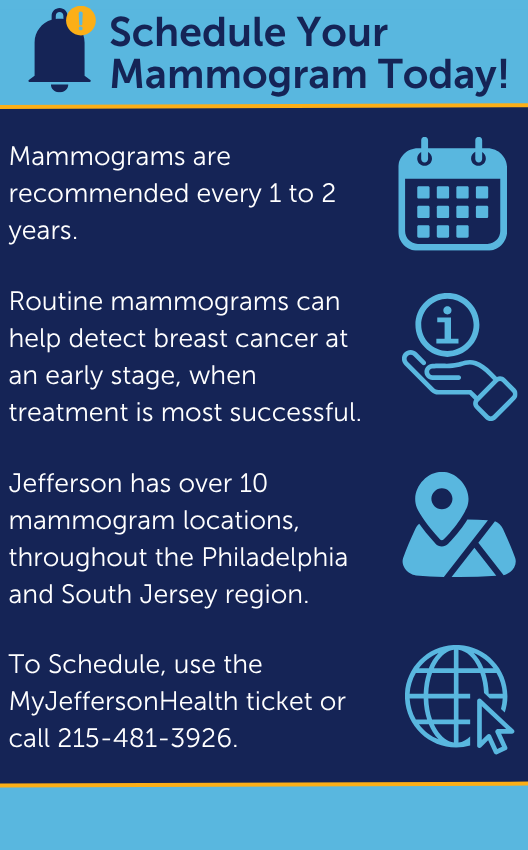
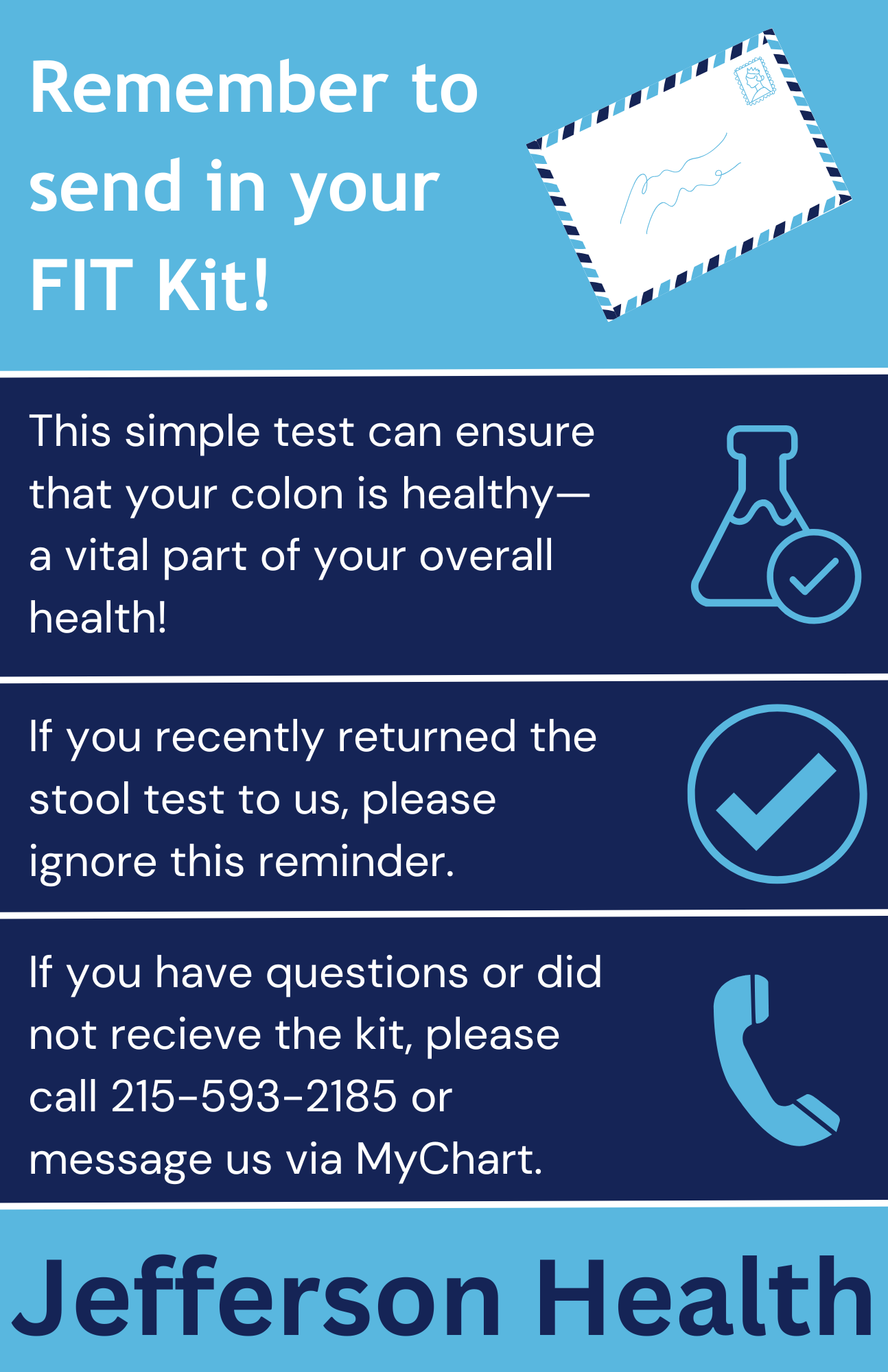
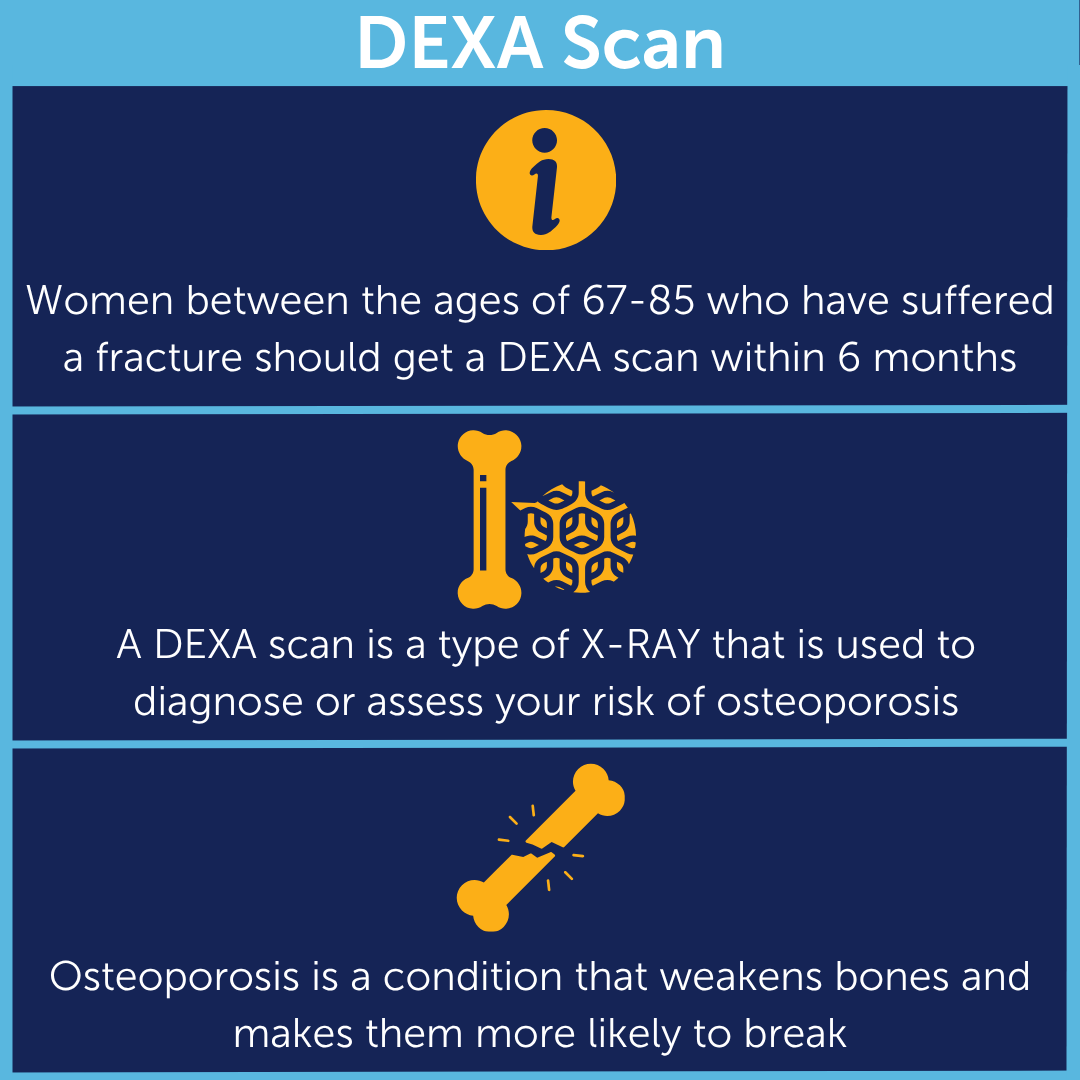
Population Health was asking people to take different next steps across recurring care gaps: schedule a mammogram, return a FIT kit, follow up on a DEXA message after a fracture, or understand what the outreach team could help arrange. Each task carried its own clinical and operational authority, but the receiving problem was familiar: a person had to recognize the subject, find the action, understand the support route, and know what would happen after responding.
Treating the message as service delivery meant making the handoff legible through approved text, visual emphasis, a delivery channel that worked on the receiving device, and a staff workflow that could be repeated without starting over. The graphic served that handoff without carrying a promise that it would change behavior.
Building inside distributed authority
The Population Health team already had workqueues and a rudimentary reusable Epic message mechanism. I learned the available Epic functionality, sought information from a capacity-constrained Epic team, and implemented the richer message layer rather than handing over a finished specification. I added reusable Epic message templates with selectable elements, links, visual assets, delivery behavior, implementation notes, and staff training. I also substantially implemented the Population Health messaging side of referral scheduling tickets, helping the team connect a MyChart scheduling ticket to a patient message, an image, or an actionable link. I did not design Jefferson's enterprise referral or scheduling-ticket capability.
The surrounding authority stayed distributed: the program manager and director managed the existing workqueues and data pulls; Marketing reviewed brand use and helped make the materials institutionally usable; Population Health leadership reviewed operational use; and the relevant clinical or program owner remained responsible for clinical wording, care-gap requirements, and approval. I contributed to the patient-facing copy, but copy development was collaborative, and I could not authorize alone the sentence a patient received.
That division made the system more useful by giving each reusable message a named source of truth, a local owner, and a clear point at which clinical judgment or a program decision took over.
A reusable library across care gaps
Across the project, I created roughly 25 reusable message or graphic assets spanning multiple care gaps. The count refers to individual reusable pieces, not 25 campaigns or complete translated families. Some Spanish variants existed, but I do not have a record of who translated or reviewed them.
The shared Canva files were generic and contained no PHI. When a message needed patient-specific context, that personalization stayed inside the authenticated Epic/MyChart workflow, keeping the repeatable design layer separate from the patient record and current clinical source.
The team installed MyChart on phones and used multiple phones and computers to send and compare demonstrations. Staff were proud to use the materials, and leaders valued the collaboration with Marketing. The implementation record contains no denominator, comparison design, measured response effect, or staff-time study from which to estimate a numeric benefit.
The visual choices were intentional rather than clinical code. Jefferson's palette supplied intentional emphasis within a branded message system; emphasis could draw attention to serious information, an actionable link, or positive news. Words, labels, links, and structure still carried the meaning without color, and current adopters must check the exported asset and its receiving surface again.
I attended the American Public Health Association's 2023 Policy Action Institute in Washington, D.C., during the project period. The event influenced how I thought about public-facing health communication. It was an influence, not a source for the complete Jefferson method or an endorsement of these materials.
Four messages, kept as historical objects
Four Jefferson-branded graphics remain from the project and appear here at their natural aspect ratios. The accompanying text describes each graphic's delivery setting and the details a current adopter would need to revalidate. Phone numbers, scheduling instructions, and care-gap wording inside the images are historical, not current calls to action.

The workflow had to carry the message
The reusable asset was only useful when the surrounding path held together. An outreach queue identified the work, a staff member made the call or left a voicemail, a reusable template supplied the approved message, an image or link supported the action, and the team documented what happened. Referral scheduling tickets gave some messages a direct operational handoff. The queue, data pull, and clinical decision did not become mine simply because I built the message layer that connected them.
The workflow reconstruction was created later to explain the pattern; its records and interface fragments are illustrative rather than a live Epic screenshot or contemporaneous project record.
Project workflow reconstruction
The reconstructed message workflow
The implemented pattern connected an existing queue to staff outreach, an approved reusable message, a supporting graphic or link, delivery, and documentation. Every visible record and interface fragment is illustrative—not a live Epic screen or patient record.
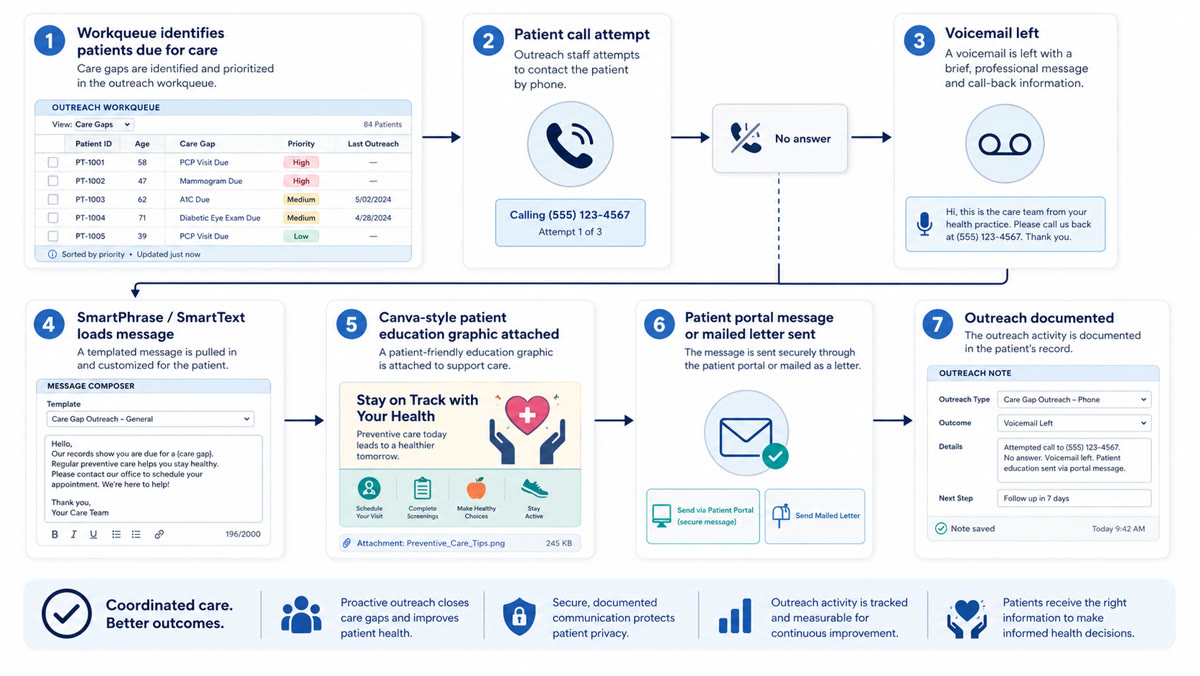
- 01Existing queue
Program leadership and managers manage the existing workqueue and underlying data pulls.
- 02Outreach contact
A staff member calls, leaves a voicemail when appropriate, and follows the local script.
- 03Reusable message
An approved Epic message template supplies complete text and selectable elements.
- 04Supporting asset
A generic, no-PHI graphic or actionable link supports the message rather than replacing it.
- 05Local delivery
The team confirms its actual MyChart, scheduling-ticket, or letter behavior before sending.
- 06Documentation
The outreach action, response, and next owner are recorded in the approved local workflow.
A reconstruction of the implemented message path. The records and interface elements are illustrative rather than live Epic screens or patient data.
Make the next local version useful
A patient-facing message works only as part of the service around it: a clear job, authorized words, a primary action, an intentional visual hierarchy, a tested receiving surface, and an owner who can answer what happens next. Each organization must configure and verify its own template objects, attachment behavior, routing, and response policy in Epic/MyChart.
The Canva-to-MyChart Field checklist provides a practical working sequence and distinguishes the Jefferson implementation from current guidance and local decisions. The colorectal screening project follows one care gap through its complete physical and clinical pathway; this project focuses on the reusable communication layer that can travel across care gaps.
Supporting documents
Carry the message system into local work
Use the checklist to define the communication job, write the complete text, pair the visual with the real delivery path, test the receiving experience, and assign the owners who keep the pattern usable.
Planning checklist
Canva-to-MyChart Field checklist
A practical, editable sequence for designing, delivering, testing, maintaining, and retiring a patient-message pattern within local communication and Epic/MyChart workflows.
Open the checklistNotes
The ONC SAFER Guide: Clinician Communication treats portal communication as a safety concern and recommends understandable content, language and literacy awareness, and clear response expectations. Jefferson's implementation history and outcomes come from the project record, not the guide.
The CDC plain-language guidance supports leading with the main message, using familiar words, and organizing copy for scanning. The Web Content Accessibility Guidelines 2.2 add text alternatives, contrast, resizing, reflow, and non-color cues. These are current practice references, not proof that a historical asset conformed everywhere.
HHS language-access guidance supports qualified interpretation or translation and meaningful access. The project record does not identify how its Spanish variants were translated or validated. MyChart's messaging help describes a non-urgent channel whose available recipients and local response policies vary by organization.
The APHA 2023 Policy Action Institute record places the event in Washington, D.C., on June 15–16, 2023 and describes its focus on policy, advocacy, and communications. Cole attended the event during the project and drew on it as an influence; Jefferson's message method was developed separately.